I don’t remember what it feels like to live without pain. At 15, I began feeling aching, stabbing, and burning sensations in my lower back and down my legs. Swallowing a few Aleve didn’t help—in fact, nothing did. If I sit or stand for any period of time, or lift something heavy or fall, I pay for it, sometimes for weeks or months. I’ve slept on the kitchen linoleum, because the carpet felt too soft to stand.
For 17 years, I went to doctor after doctor, undergoing scans, physical therapy, and just about every “alternative” treatment that promised relief. Despite some amazing doctors and the expensive tests at their disposal, they could never see anything wrong, so I never got a diagnosis.
That is, until a couple of years ago, when a routine CAT scan finally caught a structural problem with my spine. Because of that, I qualified to have a spinal cord stimulator, an electronic device used to treat chronic pain, implanted into my back. Although I was scared to go under the knife, I was more than willing to become a cyborg in order to find even partial relief. And this type of therapy might also be able to help some of the 100 million Americans who suffer from chronic pain.

According to a 2011 report from the non-profit National Academy of Medicine (formerly known as the Institute of Medicine), chronic pain affects 1.5 billion people worldwide. That’s 20 percent of all humans on Earth, more than those with heart disease, cancer, and diabetes combined, according to Abbott Laboratories. And in many cases, doctors can’t pin down a culprit.
“When neural circuits all work, it’s like a symphony,” says Dr. Allen Burton, medical director of neuromodulation at Abbott. “But sometimes, somebody inherits a bad gene, or gets injured, or something nobody knows goes amiss.” As a result of this unknown cause, certain neural circuits might start firing over and over again. Our brains think this repeated signal indicates a continuing problem. “All of a sudden, instead of having normal sensation, you have pain, or a terrible ongoing sensation that won’t go away,” Burton says.
There are many kinds of chronic pain. Sometimes, as in my case, pain pills really do help, but for other conditions, opiates just aren’t as effective as other options. So the medical establishment, and their patients, have long sought more effective pain relief without them. A spinal cord stimulator (SCS) is one of those treatments.
A SCS works by overriding the pain signals your body sends to your brain. My doctor, Raimy Amasha at Austin’s Capitol Pain Clinic, put it like this: When someone hits their funny bone, almost universally, they’ll reach over to rub their hurt elbow because it creates a nice sensation that distracts from the ache. “Your brain can only focus on so many things,” he says. “When feedback is going to the brain, the body focuses more on that pleasant feeling and essentially pushes out the channel of pain sensation.”
When a recent study examined data from opioid-using patients who received an SCS, it found that subjects who removed their system went on to take higher average daily doses of opioids than those who continued the therapy. Although this particular study comes from Abbott Laboratories, the same company that produces spinal-cord stimulators, less-invested sources are also optimistic.
“This is a new frontier for treating spinal cord injuries, in terms of being able to bypass the damaged area and restore capabilities and function,” says neurosurgeon Ali Rezai, Associate Dean of Neuroscience and Director of the Neurological Institute at The Ohio State University’s Wexner Medical Center.
That’s not to say that electrical stimulation will completely eliminate opiate use. While these drugs can cause debilitating addictions, withholding them from the people who need them most can induce incredible damage. My pain has sometimes been so great that I needed opioid medication to prevent me from sobbing and writhing and allow me to get out of bed in the morning. But needing help to control my pain does not make me an addict.
Still, doctors have been reluctant to prescribe the medication I needed for several reasons: I seemed too young to require such strong treatment, my pain got worse at night when they couldn’t see it, and I tried to maintain a positive affect (because, as a woman who grew up in the South, I was raised to smile and be polite—even when I feel at my worst).
Even with a prescription, opiates are far from the easy answer. On top of the odyssey of finding and funding health insurance, I have to pay hundreds of additional dollars to get my urine tested three to four times per year. Many states require these random reviews to demonstrate that prescription opiate users are taking their medication correctly. While Texas, where I live, doesn’t out-and-out require urine testing, it does legislate that doctors periodically “consider” doing so—and any physician who declines “must document in the medical record his or her rationale for not completing such steps.” Every patient I know is undergoing urine testing.
It costs far more than that to see my pain doctor monthly, which I must do in order to walk away with a prescription—even if my condition has not changed. And the landscape is bleak: Pain clinics are closing in droves, but nobody is accepting new patients. That means people like me have to drive hours to reach our monthly appointments.
For many, it’s not practical to get rid of opioids entirely. But it sure would be nice to be able to reduce my reliance on them, when and how my doctor and I decide.
That’s where my all-important CAT scan came in. In July 2015, Amasha told me that the two most important things on my scan were lumbosacral radiculitis and lumbosacral spinal stenosis. The bones of my spine rub against and pinch the nerves that lead to the rest of me. That causes throbbing, burning, and stabbing sensations.
For the first time in my life, I finally had a name for what was causing this pain. Even better, I eventually realized that these results put a spinal cord stimulator on the table as a real option.
Before getting a long-term implant, we had to make sure it would work for me. First, I had to do three lumbar injections of steroids to make sure the stim would be placed in the right spot. Then I got to take a trial run with the stimulator technology.
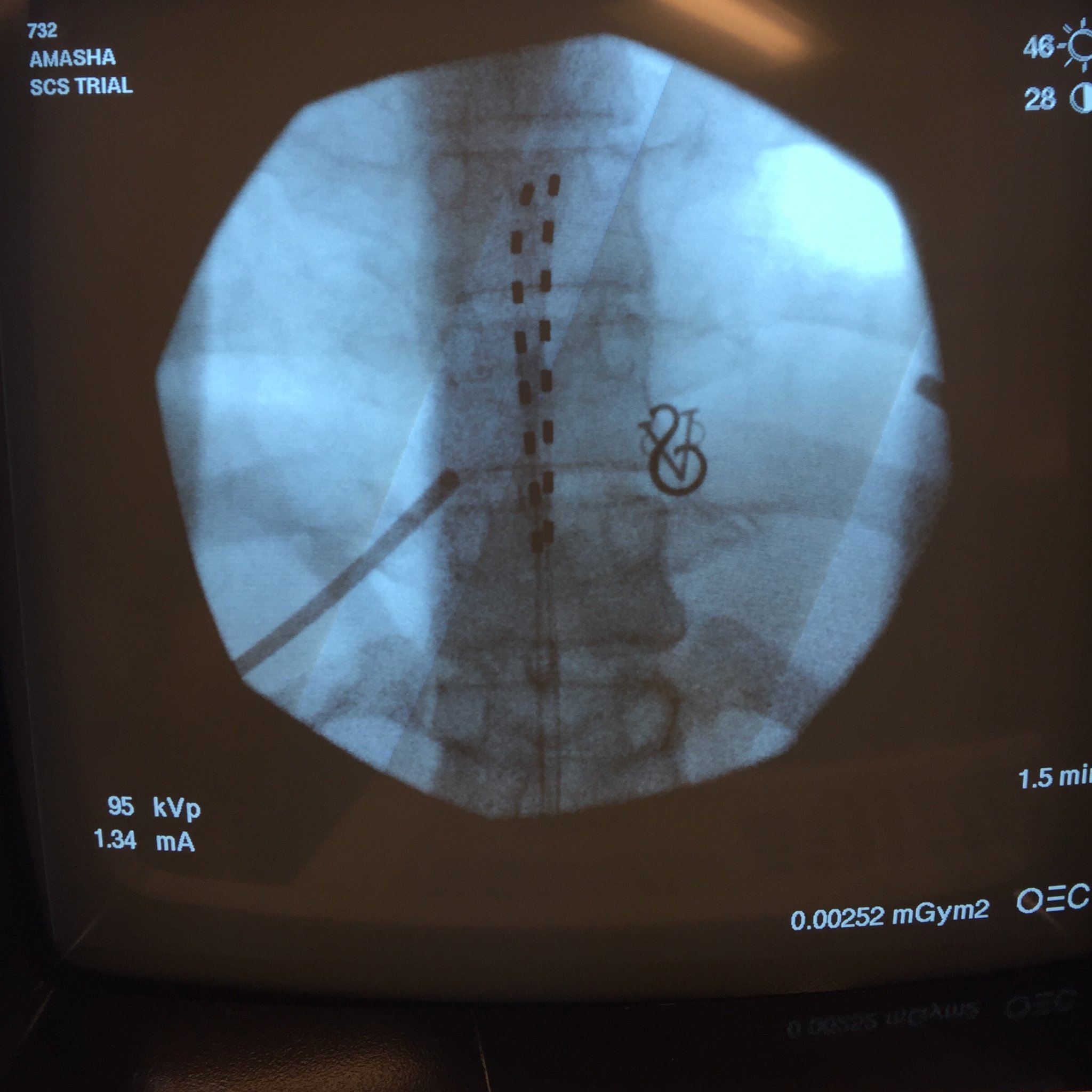
This was a try-before-you-buy treatment. Using X-ray fluoroscopy to guide a hollow needle, they insert electrodes into the space between bone and spinal cord, positioning this trial lead over specific nerves they think are causing the pain. The wires exit the body and connect to an external battery.

Doctors tape everything down very well, caution you not to shower (apologies to my husband), and give you a controller and a weird corset-like brace to hold everything in place. Then they send you home to see if it helps. I asked Timothy Deer, president and chief executive officer of The Center for Pain Relief in Charleston, West Virginia, about my chances. In his experience, someone with my diagnosis has about a 70 percent chance of the trial alleviating pain; however, he said if it did help, the odds are more like 90 percent that the actual surgery will work.
Still, I cautioned myself not to hope too much. Spinal-cord stimulation isn’t the first treatment to use electrical currents for pain relief—it’s not even the first or second I’d already tried. A very simple version of this technology, called a Transcutaneous Electrical Nerve Stimulation (TENS) unit, is available over-the-counter. (Some entrepreneurs have even created a specialized TENS unit to tackle menstrual pain.) Unfortunately, none of these less-invasive electrical techniques worked for me—electroacupuncture (where an electric current is run between acupuncture needles) was the only treatment that seemed to help at all, and even then, the benefits plateaued too quickly.
So I started my stim trial. For the next week, when I noticed the pain breaking through, I pushed a button. Instead of the pain, I felt the weird pulse of electrical current in my nerves.
Unlike my previous electrical experiences, this device actually drowned out my pain. It sent regular waves of electrical pulses through my nerves in a pattern called “tonic stimulation.” The most commonly used type of waveform technology, this feels like a continuous buzzing, or the tingles of a foot that’s fallen asleep. That’s not the most pleasant sensation, but I would trade suffering for vague buzziness any day.
Once my medical team knew a stimulator could help me, they pulled the wires out of my spine and we began talking about which product would work best for my specific issues. Abbott, Boston Scientific, and Medtronic are all manufacturing this type of device, each with its own pros and cons.
Each model has the stim itself in the spine, connected via a small wire to a small battery pack that doctors place under the fat of the hip. (I can actually reach back and feel the wire running under my skin.) Some of these battery packs can recharge wirelessly about once a week. Other models eschew rechargeables in favor of a cell that won’t need to be replaced for seven or eight years. Who knows what the pain-management landscape will look like then?
All the information felt a little overwhelming. “Because of the opiate crisis, we’re going to see more spending by investors to enhance our field farther,” says Deer. “The whole field of pain relief is better right now that it’s ever been.” That also means I had an abundance of SCS options.
After two months of research, I finally chose Abbott’s Proclaim system for a few reasons: First and foremost, my insurance covered it. It lasts up to 8 years before the battery dies (only 15 percent of SCSs have this option), it can safely go through an MRI scanner, and it accepts remote software upgrades. That means I won’t have to undergo surgery each time the technology improves. Plus, it lets you control your spinal stimulator through an iPod! (And if the iPod fails, they give you a comically large, U-shaped magnet to use as a last-resort “off” switch.)
But there was a final factor that elevated the Proclaim: It could apply a so-called burst waveform that I kept hearing the FDA would approve “any day now.” This pattern would allow me to avoid the buzzy, tingling sensations that had been the SCS norm. According to Amasha and my Abbott rep, burst stimulation better mimics the way your nerves naturally send and receive signals to make their current feel like nothing at all.
“In the last two years, neuroscience has made more progress than in all of recorded history toward understanding neural circuitry, how thoughts are processed, and different brain-disease states,” says Burton. “This burst stimulator fits into that progress: We’re right on the cusp of taking the knowledge that these scientists are getting and translating it into treatments that help people.”

Surgery day came and went, followed by a few days of recovery. Finally, I returned to Amasha’s office, terrified but hopeful, to have my stim turned on for the first time. There, my husband and I met with our Abbott representative, expecting to experience the tonic waveform I’d used in my trial.
“Would you like to try the burst waveform? It just got approved by the FDA,” he said, adding that I’d be the first person in the Austin, Texas area to use this technology. He pulled out an iPad and started tapping away at his Clinician programing app. Within minutes, he had turned on my stim and handed me the sixth-generation iPod Touch that would, from that point forward, control the tech in my back. (I immediately dubbed mine the SpinePod.)
You know how you feel when you drink a shot of espresso, or your Advil kicks in, or you stand up straight and square your shoulders? Imagine that sensation of relief, but confined to your lower back. Turning on the burst stimulation in my device makes me feel like my foundations have shifted to a more secure footing. It feels like nothing—but a nothing that pushes the pain down.
Other painkillers distance me from the pain or cushion me from it, and that’s valuable. But it’s always lurking behind me. This isn’t like that at all. Unlike with the other treatments, there’s no promise of future agony. The SCS folds my pain up like complex origami, creasing and accordioning.
More than one year later, the SCS continues to banish much of my pain. The only side effect was that it also improved my mood—more than could be explained by just a lack of pain. The week after I began to use my spinal stimulator, my husband commented, “I don’t know if it’s the Burst or not, but you seem calmer than I’ve ever seen you.” According to a study assessing the Burst waveform, “It is specifically capable of influencing the affective/attentional components of pain.” In other words, the effect on my mood is real.
But in my delight over the effectiveness of the SCS, I’m still well aware that I’m incredibly lucky to have this pain treatment option. My doctors happened to see something on a CAT scan for the first time ever; I found a good pain-management doctor who really listens to me and treats me as an equal; I had pretty good insurance (a huge concern, especially for women and people with preexisting conditions); and all the tests and trials drew to an end right as the FDA approved the burst waveform. Most of all, my family and I had enough money. I got to try out all those treatments, pay for the diagnostic injections, and purchase the back brace, cane, and absurdly expensive medication I needed. Insurance covered the six-figure stim, but I had the resources to meet my ridiculous deductible before that happened. Many people lack those resources.
Even for me, the battle is not over. Since this surgery I’ve actually had another disc herniate, complicating everything. My spine isn’t cured, and I still hurt all the time. But the pain is far more controlled, and I can function much better at my current level of discomfort. Since getting the stim, I got married, started a new part-time job advocating for people in chronic pain, and I feel like I can cautiously, but realistically, try to plan a life. For the first time in a long time, tomorrow looks better than yesterday.
